Assess the effectiveness of structured of teaching programme on knowledge and practice regarding life style modifications among coronary artery disease patients at PES hospital in Kuppam
Year: 2025; Volume: 5; Issue: 2; Page No: 3 – 8
Article Type: Original Article
Authors: Daniel Arun Kumar1*![]() , Abhirami M2, Sumitha Devi3, Sreedevi TK4, Pavithra MN5, Melvin David6, Alphonsa Thomas7, Alluri Swapha Priya8, Anakha Benny9, Aneetta James10, Anju Saju11
, Abhirami M2, Sumitha Devi3, Sreedevi TK4, Pavithra MN5, Melvin David6, Alphonsa Thomas7, Alluri Swapha Priya8, Anakha Benny9, Aneetta James10, Anju Saju11
![]() https://doi.org/10.55349/ijmsnr.20255238
https://doi.org/10.55349/ijmsnr.20255238
Affiliations:
1Professor, Department of Medical Surgical Nursing, PES College of Nursing, Andhra Pradesh.
2Professor, 3Professor, Department of Mental Health Nursing, PES College of Nursing, Andhra Pradesh.
4Associate Professor, Department of Mental Health Nursing, PES College of Nursing, Andhra Pradesh.
5Associate Professor, Department of Obstretics & Gynaecology Nursing, PES College of Nursing, Andhra Pradesh.
6Assistant Professor, Department of Community Health Nursing, PES College of Nursing, Andhra Pradesh.
7, 8, 9, 10, 11 4th Year B.Sc. Nursing Students, PES College of Nursing, Andhra Pradesh.
|
How to cite this article: Daniel AKK, Abhirami M, Devi S, Sreedevi TK, Pavithra MN, David M, Thomas A, Priya AS, Benny A, James A, Saju A. Assess the effectiveness of structured of teaching programme on knowledge and practice regarding life style modifications among coronary artery disease patients at PES hospital in Kuppam. Int J Med Sci and Nurs Res 2025;5(2):3–8. DOI: https://doi.org/10.55349/ijmsnr.20255238 |
Corresponding Author:
Prof. K. Daniel Arun Kumar,
Professor, Dept. of Medical Surgical Nursing,
PES College of Nursing,
Kuppam, Andra Pradesh, India.
Email ID: samuraidaniel432@gmail.com
Article Summary: Submitted: 07-April-2025 Revised: 30-April-2025 Accepted: 18-May-2025 Published: 30-June-2025
Abstract
Background: Cardiovascular diseases (CVDs) remain the leading cause of mortality worldwide, accounting for approximately 17.1 million deaths annually. Coronary artery disease (CAD), including myocardial infarction, angina pectoris, and atherosclerotic cardiovascular disease, is a significant contributor to this burden.
Methods: Structured Teaching Programmes (STPs) are educational strategies aimed at enhancing patient knowledge and promoting healthy behavior adoption. This pre-experimental study assessed the effectiveness of an STP on lifestyle modifications among CAD patients admitted to the Coronary Care Unit of PES General Hospital, Kuppam. Andhra Pradesh.
Results: A total of 30 patients were selected using a convenient sampling technique. Findings showed that in the pre-test, 90% of participants had inadequate knowledge, which improved significantly in the post-test, where 50% attained moderate knowledge. The mean knowledge score increased from 6.63 (SD = 3.90) to 15.10 (SD = 3.04). In terms of practice, 43.3% showed adequate practice in the pre-test, which also improved post-intervention. A significant association was observed between pre-test knowledge scores and religion (p<0.001), while other demographic variables were not statistically significant.
Conclusion: The study concludes that the STP effectively improved knowledge and practice regarding lifestyle modifications among CAD patients, highlighting the value of structured educational interventions in cardiac care.
Keywords: cardiovascular diseases, coronary artery disease, life style modifications, patients
Full Text
Introduction
Coronary artery disease (CAD) remains one of the leading causes of morbidity and mortality worldwide. It is a condition characterized by the narrowing or blockage of coronary arteries due to the build-up of atherosclerotic plaques, leading to reduced blood flow to the heart muscle. This can result in chest pain (angina), shortness of breath, myocardial infarction (heart attack), and even sudden death. According to the World Health Organization (WHO), cardiovascular diseases, including CAD, account for approximately 31% of all global deaths (WHO, 2021). [1] cardiovascular diseases are the world’s largest killers, claiming 17.1 million lives a year. Tobacco use, an unhealthy diet, physical inactivity, and harmful use of alcohol increase the risk of cardiovascular diseases. CAD which encompasses Acute Myocardial infarction, Angina pectoris, and Atherosclerotic cardiovascular disease is the leading cause of death in the industrialized world. [2] Approximately two out of every three incidents of myocardial infarction (MI) occur without warning and of note, one third of first MIs are fatal; 20% of patients die out of hospital and 13% die within the first 24 to 48 hours of hospitalization. [3] Lifestyle modifications are critical in the management and prevention of CAD. Evidence suggests that adopting healthy behaviors such as a balanced diet, regular physical activity, smoking cessation, stress management, and adherence to prescribed medications can significantly reduce the risk of disease progression and improve overall cardiovascular health (American Heart Association, 2020). [4] Despite the known benefits, many patients with CAD struggle to implement and maintain these lifestyle changes. A study by Chow et al. found that only a small recommended lifestyle modifications, underscoring the need for effective educational interventions.[4] Educational interventions, particularly structured teaching Programmes (STP), play a vital role in enhancing patients’ knowledge and encouraging the adoption of healthy practices. These Programmes are designed to provide comprehensive and systematic information tailored to the needs of CAD patients. By improving patients’ understanding of their condition and the importance of lifestyle modifications, STPs aim to empower individuals to take an active role in managing their health. A meta-analysis by Clark et al. (2012) demonstrated that patient education significantly improves adherence to lifestyle modifications and clinical outcomes in CAD patients. The main objectives to assess the pre-test and post-test level of knowledge and practice, to assess the effectiveness of STP by comparing pre-test and post-test level of knowledge and practice and to associate the pre-test level of knowledge and practice with their selected demographic variables.
Materials and Methods
A Quantitate pre-experimental study was conducted in December 2024 among 30 CAD patient who got admitted in Critical care Unit with the diagnosis of Coronary Artery Disease at PES Hospital were selected by using convenient sampling technique, informed consent were taken before the study, patients’ knowledge and practice were assessed by using structured self-administered questionnaire. This includes demographic variables and questionnaire on knowledge and practice regarding life style modifications among coronary artery disease patient.
Statistical Analysis: Collected data were compiled using Microsoft Excel 2013 and data were analyzed by SPSS 14.0 version. Categorical data were presented as frequency and proportions and Continuous variables were as mean and standard deviation. Association between pre-test level of knowledge with their selected demographic variables was analyzed by Chi-Square test.
Results
The demographic characteristics of coronary artery disease (CAD) patients. The majority (36.7%) were aged 61–65 years. Most were male (66.6%), and 40% were illiterate, while 56.7% had primary education. Regarding occupation, 46.7% were moderate workers. A majority (56.7%) identified as Hindu, followed by Muslims (33.3%) and Christians (10%). Half of the participants (50%) resided in rural areas, and 83.3% were non-vegetarians. About 33.3% reported smoking, 13.3% consumed alcohol, and 53.3% had other habits. Clinically, 60% had myocardial infarction, 16.7% had angina, 16.7% had coronary atherosclerosis, and 6.7% had other forms of CAD as shown in Table-1.
Table – 1 Distribution of Neurobiological mechanisms of post-MI depression [21]
| S. No | Demographic Variables | Classifications | No. of Patients | Percentage |
| 1 | Age Groups | a) 45 – 50 | 6 | 20.0 |
| b) 51 – 55 | 7 | 23.3 | ||
| c) 56 – 60 | 6 | 20.0 | ||
| d) 61 – 65 | 11 | 36.7 | ||
| 2 | Gender | a) Male | 20 | 66.7 |
| b) Female | 10 | 33.3 | ||
| 3 | Educational Status | a) Illiterate | 12 | 40.0 |
| b) Primary education | 17 | 56.7 | ||
| C c) Secondary Education | 0 | 0 | ||
| D d) Higher Secondary Education | 0 | 0 | ||
| e) Under graduation | 0 | 0 | ||
| f) Post-Graduation | 1 | 3.3 | ||
| 4 | Occupation | a) Sedentary worker | 8 | 26.7 |
| b) Moderate Worker | 14 | 46.7 | ||
| c) Heavy Worker | 8 | 26.7 | ||
| 5 | Religion | a) Hindu | 17 | 56.7 |
| b) Muslim | 10 | 33.3 | ||
| c) Christian | 3 | 10.0 | ||
| 6 | Area of Residence | a) Rural | 15 | 50.0 |
| b) Urban | 10 | 33.3 | ||
| c) semi urban | 5 | 16.7 | ||
| 7 | Dietary pattern | a) Vegetarian | 5 | 16.7 |
| b) Non vegetarian | 25 | 83.3 | ||
| 8 | Habits | a) smoking | 10 | 33.3 |
| b) alcohol | 4 | 13.3 | ||
| c) others specify | 16 | 53.3 | ||
| 9 | Type of CAD | a) MI | 18 | 60.0 |
| b) Angina | 5 | 16.7 | ||
| c) Coronary atherosclerosis | 5 | 16.7 | ||
| d) Others specify | 2 | 6.7 |
Table–2 Frequency and percentage distribution of the pre-test level of knowledge among coronary artery patients. (N=30)
| Level of Knowledge | Frequency | Percentage |
| Adequate Knowledge | 1 | 3.3 |
| Moderate Knowledge | 2 | 6.7 |
| In adequate Knowledge | 27 | 90.0 |
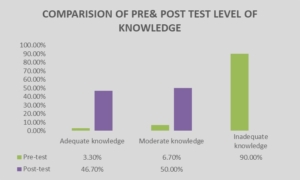
1 (3.3%) coronary artery patients were had adequate knowledge, 2 (6.7 %) were had Moderate Knowledge and 27 (90.0%) were had inadequate Knowledge. [Table – 2]
Table–3 Frequency and percentage distribution of the post-test level of knowledge among coronary artery patients (N=30)
| Level of Knowledge | Frequency | Percentage |
| Adequate Knowledge | 14 | 46.7 |
| Moderate Knowledge | 15 | 50 |
| In adequate Knowledge | 1 | 3.3 |
Majority 14(46.7%) coronary artery patient were had adequate knowledge, 15(50.0%) were had in Moderate Knowledge and 1 (3.3%) were had in adequate Knowledge [Table – 3]
Table: 4 – Comparison of pre-test and post-test knowledge mean and SD among cataract patient
| –
Post-Test knowledge
|
Frequency | Percentage |
| Adequate practice | 13 | 43.3 |
| In adequate practice | 17 | 56.7 |
Majority 13 (43.3%) coronary artery patient were had adequate practice, 17 (56.7%) were had in adequate. [Table – 4]
Figure–1 Comparison of frequency and percentage distribution of pre-test and post-test level of Knowledge among of the coronary artery patients.
Table–5 Frequency and percentage distribution of the post-test level of practice among coronary artery Disease patients
| Level of Practice | Frequency | Percentage |
| Adequate Practice | 20 | 66.7 |
| In Adequate Practice | 10 | 33.3 |
Majority 20 (66.7%) coronary artery patient were had adequate practice, 10 (33.3%) were had in adequate Practice [Table-5]
Figure–2 Comparison of frequency and percentage distribution of pre-test and post-test level of practice among of the coronary artery Disease patients

Association of pre-test scores of knowledges on life style modification among coronary artery patients with their selected demographic variables Religion was significant at the level of p<0.001 respectively. Other variables like Age, Sex, Educational Status, Occupation, Area of Residence Dietary Pattern, Habit and Type of CAD weren’t significant [Figure–2]
Table – 6 Association of pre-test level of knowledge among CAD patients with their selected demographic variables
|
S. No |
Demographic Variables |
Classifications |
Level of Knowledge | Chi-square Value | p-Value | ||
| In adequate Knowledge | Moderate Knowledge | Adequate knowledge | |||||
|
1 |
Age | a) 45-50 years | 4 | 2 | 0 | 12.59 |
0.050 NS |
| b) 51-55 years | 7 | 0 | 0 | ||||
| c) 55-60 years | 5 | 0 | 1 | ||||
| d) 60-65 years | 11 | 0 | 0 | ||||
|
2 |
Sex |
a) Male | 18 | 1 | 1 | 0.750 | 0.687
NS |
| B) Female | 9 | 1 | 0 | ||||
|
3 |
Educational status |
a) Illiterate | 11 | 1 | 0 | 0.918 | 0.922
NS |
| b) Primary education | 15 | 1 | 1 | ||||
| c) Secondary education | 0 | 0 | 0 | ||||
| d) Higher secondary education | 0 | 0 | 0 | ||||
| e) Under graduate | 0 | 0 | 0 | ||||
| f) Post graduate | 1 | 0 | 0 | ||||
|
4 |
Occupation |
a) Sedandry Worker | 5 | 2 | 1 | 9.167 | 0.057
NS |
| b) Moderate Worker | 14 | 0 | 0 | ||||
| c) Heavy Worker | 8 | 0 | 0 | ||||
|
5 |
Religion |
a) Hindu | 16 | 1 | 0 | 9.596 | 0.48
S* |
| b) Muslim | 9 | 1 | 0 | ||||
| c) Christian | 2 | 0 | 1 | ||||
| 6 | Area of Residence | a) Rural | 14 | 1 | 0 | 4.074 | 0.396
NS |
| b) Urban | 9 | 0 | 1 | ||||
| c) Semi Urban | 4 | 1 | 0 | ||||
| 7 | Dietary Pattern | a) Vegetarian | 4 | 1 | 0 | 1.867 | 0.393
NS |
| b) Non vegetarian | 23 | 1 | 1 | ||||
|
8 |
Habit |
a) smoking | 8 | 1 | 1 | 2.618 | 0.624
NS |
| b) alcohol | 4 | 0 | 0 | ||||
| c) others specify | 15 | 1 | 0 | ||||
|
9
|
Type of CAD | a) MI | 15 | 2 | 1 | 2.222 | 0.898
NS |
| b) Angina | 5 | 0 | 0 | ||||
| c) Coronary atherosclerosis | 5 | 0 | 0 | ||||
| d) Others specify | 2 | 0 | 0 | ||||
The association of pre-test scores of knowledges on life style modification among coronary artery patients with their selected demographic variables Religion was significant at the level of p<0.001 respectively. Other variables such as Age, Sex, Educational Status, Occupation, Area of Residence Dietary Pattern, Habit and Type of CAD were not significant. [Table – 6]
Table: 7 Association of pre-test level of practice among CAD patients with their selected demographic variables
| S. No | Demographic
Variables |
Classifications |
Level of Practice | Chi-square
Value |
p-Value | |
| In Adequate
Practice |
Adequate Practice |
|||||
| 1 | Age | a) 45-50 years | 2 | 4 | 2.595 | 0.458
NS |
| b) 51-55 years | 4 | 3 | ||||
| c) 55-60 years | 3 | 3 | ||||
| d) 60-65 years | 8 | 3 | ||||
| 2 | Sex | a) Male | 10 | 10 | 1.806 | 0.259
NS |
| b) Female | 7 | 3 | ||||
| 3 | Educational status | a) Illiterate | 7 | 5 | 0.874 | 0.646
NS |
| b) Primary education | 9 | 8 | ||||
| c) Secondary education | 1 | 0 | ||||
| d) Higher secondary education | 0 | 0 | ||||
| e) Under graduate | 0 | 0 | ||||
| f) Post graduate | 0 | 0 | ||||
| 4 | Occupation | a) Sedandry Worker | 4 | 4 | 0.621 | 0.733
NS |
| b) Moderate Worker | 9 | 5 | ||||
| c) Heavy Worker | 4 | 4 | ||||
| 5 | Religion | a) Hindu | 11 | 6 | 1.701 | 0.427
NS |
| b) Muslim | 4 | 6 | ||||
| c) Christian | 2 | 1 | ||||
| 6 | Area of Residence | a) Rural | 7 | 8 | 1.357 | 0.507
NS |
| b) Urban | 7 | 3 | ||||
| c) Semi Urban | 3 | 2 | ||||
| 7 | Dietary Pattern | a) Vegetarian | 4 | 1 | 1.330 | 0.261
NS |
| b) Non vegetarian | 13 | 12 | ||||
| 8 | Habit | a) Smoking | 4 | 6 | 2.155 | 0.340
NS |
| b) Alcohol | 2 | 2 | ||||
| c) Others specify | 11 | 5 | ||||
| 9 | Type of CAD | a) MI | 12 | 6 | 3.937 | 0.268
NS |
| b) Angina | 2 | 3 | ||||
| c) Coronary atherosclerosis | 3 | 2 | ||||
| d) Others specify | 0 | 2 | ||||
The association of pre-test scores of Practice on life style modification among coronary artery patients with their selected demographic variables such as age, sex, educational status, occupation, religion, area of residence dietary pattern, habit and type of CAD were not significant. [Table – 7]
Discussion
In the present study aimed to assess the knowledge and practice regarding lifestyle modification among coronary artery disease patients in a selected tertiary care hospital at Kuppam, Chittoor District. Andhra Pradesh. Demographic data revealed that most patients were aged 61–65 years, most of them66.6% were male, and 40% were illiterate. Most were moderate workers, ½ of them practiced Hinduism, 50% resided in rural areas, and 3/4th of them were non-vegetarians. A significant portion half of the patients reported other lifestyle habits. In the pre-test, most of them90% of patient’s demonstrated inadequate knowledge regarding lifestyle modification, while very less number patients had moderate knowledge, and only very little had adequate knowledge. Post-test results showed improvement, with nearly half of the study participants achieving adequate knowledge, half of the population demonstrating moderate knowledge, and only very few were remaining in the inadequate category. Pré-test practice scores indicated that nearly half of patients had adequate practice, while half of the patients had inadequate practice. Post-test results showed improvement, with demonstrating adequate practice and 33.3% reporting inadequate practice. Statistical analysis revealed a significant association between religion and pre-test knowledge scores. No significant association was observed between pre-test knowledge or practice scores and other demographic variables such as age, sex, educational status, and occupation, area of residence, dietary pattern, habits, and type of CAD. These findings are supported by a similar study conducted by Reena Isaac et al. conducted a descriptive survey to assess knowledge and lifestyle practices regarding coronary artery disease among one hundred and two women aged 35–55 in Kerala. Most participants were aged 35–39, more than 1/2th of the patients had 10th standard education, and above 50% were household workers. Overall, few had excellent, 3/4th was average, and nearly 1/4th was had poor knowledge. Knowledge was lower in areas like risk factors and diagnosis/treatment, but higher for symptoms and lifestyle changes. Regarding lifestyle practices, more than half of the patients had good practice, 3/4th was had very good practice, and few of them had average practices. Poorer scores were seen in diet in more than half and physical activity. Education level was significantly associated with knowledge. [5]
Conclusion
The study found that the majority of patients with coronary artery disease originally lacked the necessary skills and knowledge to make lifestyle changes. On the other hand, the organized training program markedly raised sufficient scores after the intervention, demonstrating a considerable improvement in both knowledge and practice levels. Other factors did not significantly affect pre-test knowledge levels, although demographic factors such as religion did. This emphasizes the necessity of focused educational interventions to successfully close knowledge and practice gaps. The findings highlight how crucial organized educational initiatives are in encouraging patients to lead healthier lives, which will ultimately enhance illness treatment and results.
Source of funding: None
Conflict of Interest: Nothing declared by the authors
Authors’ Contributions: All authors conceived and designed the article. Wrote the full paper and checked by all the authors.
Acknowledgement: We acknowledge all the CAD patients who actively participated in the study.
References
- World Health Organization. Cardiovascular diseases (CVDs) 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) [Last Accessed On: 20th February 2025]
- Bansal A, Hiwale K. Updates in the Management of Coronary Artery Disease: A Review Article 2023;15(12):e50644. DOI: https://doi.org/7759/cureus.50644 PMID: 38229816
- A Study To Evaluate The Effectiveness Of Structured Teaching Programme (Stp) On Knowledge Regarding Prevention Of Cornonary Artery Disease Among Hypertensive Patients Admitted In Kle Dr. Prabhakar Kore Hospital, Belagavi. Educational Administration: Theory and Practice. 2024;30(5):8784–8798. Available from: https://kuey.net/index.php/kuey/article/view/4461
- American Heart Association. Lifestyle Changes for Heart Attack Prevention. Retrieved from AHA. 2025. Available from: https://www.heart.org/en/health-topics/heart-attack/life-after-a-heart-attack/lifestyle-changes-for-heart-attack-prevention [Last Accessed On: 25th February 2025]
- Reena Issac, Sreedevi tr knowledge, lifestyle practices and selected modifiable risk factors of coronary artery disease. 2022;11(12):60–64. DOI: https://doi.org/10.36106/ijsr/3011185
![]() This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑Non-Commercial‑ShareAlike 4.0 International License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given, and the new creations are licensed under the identical terms.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑Non-Commercial‑ShareAlike 4.0 International License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given, and the new creations are licensed under the identical terms.