Article Type: Original Article
Title: A Clinico Pathological Correlation of FNAC and Histopathology of Thyroid Swellings: A Hospital-Based Prospective Study
Year: 2022; Volume: 2; Issue: 2; Page No: 14 – 17
Authors: Neethu Priya K*![]()
![]() https://doi.org/10.55349/ijmsnr.2022221417
https://doi.org/10.55349/ijmsnr.2022221417
Affiliations: ENT Surgeon, All India Institute of Speech and Hearing, Mysore, Karnataka, India.
Article Summary: Submitted: 20-April-2022; Revised: 21-May-2022; Accepted: 05-June-2022; Published: 30-June-2022
Corresponding Author:
Dr. Neethu Priya K
A-501, Mittal Pride Apartments,
Manadavadi Road,
Mysore,
Karnataka,
India.
Email ID: neethupriyak@gmail.com
Abstract:
Background: Fine needle aspiration cytology is a diagnostic tool in which cells are extracted from palpable swelling using FNAC gun or syringe and needle. It is a simple, speedy, safe, cost effective and accurate technique being used worldwide. But, pitfalls come along making the correlation with histopathology often necessary.
Materials and Methods: This study was a prospective study conducted among 30 patients undergoing thyroidectomy for thyroid swellings in ENT department, Bangalore Medical College and Research Institute, Bangalore. Patients were evaluated by detailed history, clinical examination, preoperative FNAC, thyroid function tests.
Results: Thirty patients who underwent thyroidectomy for thyroid swelling during the study period was selected. Among 30 cases all specimen was sent for gross and microscopic examination. Two cases of malignant neoplasms were detected, one of which was benign according to FNAC. Most common lesion was multinodular goiter. Correlation of FNAC and histopathology for benign and malignant lesions, sensitivity of FNAC was found to be 50%, specificity 100%, negative predictive value of 96.5 % and positive predictive value of 100%. p-value<0.01, showing that there is a strong positive correlation between FNAC and histopathology findings.
Conclusion: Thyroid pathologies are frequently encountered in otolaryngology clinics. Often the initial FNAC is a cost effective and minimally invasive procedure for the preoperative assessment of patients with thyroid swelling. Even though the clinical presentation may be similar in benign and malignant thyroid swellings, FNAC is the key to initial evaluation of thyroid swellings as well as to plan the surgery.
Keywords: Fine Needle Aspiration Cytology, Histopathology, Thyroid swellings.
Full Text
Introduction
Thyroid swellings are frequently encountered in clinical practice. [1] Clinical evaluation helps in diagnosis of nature of swellings, but it is difficult to distinguish early malignant lesions from more prevalent benign goitres. Ultrasonography can only distinguish solid from cystic lesions. Post-operative histopathologic examination is the only means by which precise diagnosis of swelling could be made. [2] An alternative approach other than operative is Fine Needle Aspiration Cytology. Fine needle aspiration cytology is a diagnostic tool in which cells are extracted from palpable swelling using FNAC gun or syringe and needle. It is a simple, speedy, safe, cost effective and accurate technique being used worldwide. But, pitfalls come along. Approximately 15% of all aspirates are inadequate or non-diagnostic. Respiration is critical as non-diagnostic should never be interpreted as negative for carcinoma. [3]
Evaluating the reliability of FNAC by comparing with histopathological diagnosis to evaluate sensitivity and specificity, there by its role in pre-operative diagnosis of thyroid swelling and planning proper management. The main objective of our present study to find the reliability of FNAC in the diagnosis of thyroid swellings by studying the sensitivity, specificity and positive predictive value of FNAC and to compare it with previous studies and to determine the role of FNAC in the evaluation and planning of management in thyroid swelling.
Materials and Methods
This study was a prospective study conducted in patients undergoing thyroidectomy for thyroid swellings in Sri Venkateshwara ENT Institute and Bowring and Lady Curzon Hospital, Bangalore Medical College and Research Institute, Bangalore.
Thirty patients who underwent thyroidectomy for thyroid swelling during the study period was selected. [4] Patients were evaluated by detailed history, clinical examination, preoperative FNAC, thyroid function tests. After getting informed written consent and preoperative counseling, thyroidectomy was done. The specimen was subjected to histopathological examination. Both Gross and microscopic examination was done. All details were documented in proforma including patient details, symptoms, instigation reports, FNAC and histopathology reports, surgical procedure and post-operative follow up. Data were entered and complied by using Microsoft Excel 2010 [Microsoft Ltd. USA] and analyzed using SPSS 16.0 version [IBM Ltd., USA]. Categorical variables were expressed as frequency and percentages. [5] Finding the accuracy of FNAC.
Results
A total of 30 patients who underwent thyroidectomy was included in the study. FNAC was done for all the patients. Smears obtained were adequate in all the cases and all 30 were available for histopathological examination. Age group in the current study ranged between 18 to 80 years with mean of 36.07as shown in Figure – 1. We found that majority of patients (36.7%) were in the age group 20-30 years.
Figure – 1 Distribution of Age groups among thyroidectomy patients
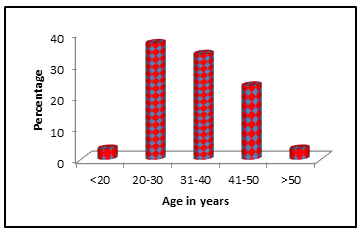
This age range and mean incidence is slightly lower as compared with previous studies [6 – 8] Gupta et al [9] reported mean age group to be 38.7 years and age of the patients ranged from 22 to 58 years.
Among 30 patients’ majority were females 87%. This showed that thyroid swellings were 6.5 times common in females than males. This was comparable to the study by Tabaqchali [10] on 239 patients where 89.1% of the cases were females and 10.9% males.
Examination revealed the most common presentation to be multinodular goitre followed by solitary nodule as shown in Figure – 2.
Figure – 2 Distribution of findings of clinical examination among thyroidectomy patients

Histopathological Findings: Maximum number of cases of nodular goitre was reported in the current study. Colloid goitre was the most common thyroid swelling in various studies. Only 6.6% of total cases reported were malignant. The most common histopathological finding was nodular and colloid goitre (62.8%), while malignancy accounted for 17.7%.
Discussion
The age range and mean incidence is slightly lower as compared with previous studies. Gupta et al [9] reported mean age group to be 38.7 years and age of the patients ranged from 22 to 58 years. The sex incidence of the patients was comparable to the study by Tabaqchali [10] on 239 patients where 89.1% of the cases were females and 10.9% males.
Comparison of histopathological findings [11]
Table – 1 Comparison of histopathological findings between current study and other studies
| HPE | Percentages | ||
| Current study | Yoo C et al12 | Kiran Rao13 | |
| MNG | 46.7 | 22.2 | – |
| Colloid Cyst | 20.0 | – | 40 |
| Hashimotos thyroiditis | 16.7 | 2.8 | 2 |
| PTC | 6.7 | 5.6 | 8 |
| Lymphocytic thyroiditis | 10.0 | – | – |
| Follicular adenoma | – | 55.6 | 25 |
| Follicular carcinoma | – | 5.6 | 11 |
| Hurthle cell adenoma | – | 8.3 | – |
| Granuloma | – | – | 10 |
Comparison of the studies by Yoo et al. [12] and Rao et al. [13] studies with our present study as shown in Table – 1
Sensitivity, specificity and Accuracy
Unsatisfactory sampling was not reported in any of the aspirations done. Where as in studies by Tabaqchali et al [10] the unsatisfactory sample rate was 43.1% on initial aspiration which was reduced to 32.2% on repeated aspiration. Correlation of FNAC and histopathology for benign and malignant lesions, sensitivity of FNAC was found to be 50%, specificity 100%, negative predictive value of 96.5 % and positive predictive value of 100%. Sensitivity of 66% and specificity of 100 % was reported by Bagga et al. [14]
A diagnostic accuracy of FNAC for thyroid was only of 69.5% according to Yoo et al. [12] The diagnostic accuracy of FNAC for thyroid swellings in this series was 96.6%. This is comparable with that of Grant has revealed that 92.86 %. [15]
False negative results of FNAC
False negative rate was 3.33% in this study for malignancy diagnosis. Various studies show false negative values varying from 1 to 11%.
FNAC finding of Nodular goitre, on Histopathological examination proved to be MNG with foci of micro papillary carcinoma. This could be possibly due to the presence of cysic spaces in papillary carcinoma or inadequate smears when small foci of micro papillary carcinoma aspirate were missed. [16]
This can be avoided by
(1). Aspirations performed in different sites of the nodule would contribute to obtain a more representative specimen.
(2). In the absence of suspicious clinical changes and with at least three FNAs confirming the cytologic diagnosis of benignity, the follow-up of nodules by FNA could be discontinued.
(3). The diagnostic change from benign to malignant after three repeat FNAs appears to indicate that it would be advisable to perform three procedures.
False positive results
In this study there were no false positive cases. A false positive rate of 6% was reported by Ylagan et al. [17] False positives were less frequent than false negatives. The false positive rate due to interpretation error in 6% cases were explained by the occurrence of overlapping cytological features among adenomatous nodules, follicular neoplasms, the follicular variant of papillary thyroid carcinoma and hashimoto’s thyroiditis.
According to Handa et al [18] five cases diagnosed colloid goiter with cystic degeneration on cytological investigation, on histological examination, four of these were diagnosed as follicular adenomas while one case was diagnosed as Hurthle cell adenoma with cystic change. This was explained on the because of the sampling of areas of cystic change rather than cellular areas. Marked cellularity of the smear also can be a problem inherent in thyroid FNA cytology. Increased cellularity of the smear and loss of cohesion may be present in hyperplastic/adenomatous goiter, adenoma, or in carcinoma
Conclusion
Thyroid pathologies are frequently encountered in otolaryngology clinics. Often the initial FNAC is a cost effective and minimally invasive procedure for the preoperative assessment of patients with thyroid swelling. Even though the clinical presentation may be similar in benign and malignant thyroid swellings, FNAC is the key to initial evaluation of thyroid swellings as well as to plan the surgery.
Often cystic lesions are the cause for inadequate sampling and false negative results. In the current study even though FNAC showed high false negative rates, the specificity and accuracy was high. Thus for planning the surgical management, FNAC proves to be highly valid. Low rate of false positive and false negative case can be achieved by applying strict criteria for specimen adequacy. Multiple aspirates have shown to reduce the false negative rate and increase the sensitivity. Also image guidance has shown to improve the adequacy of specimen sampling. To conclude FNAC is a simple and cost effective investigation for thyroid swellings. But fallacies occur, which can be overcome by combined decision by pathologist and the surgeon.
Author Contributions: NP – Conceived and designed the analysis, collected the data, performed the analysis, wrote the paper, guided throughout the process, contributed data or analysis tools, wrote and checked the article.
NP – Neethu Priya
Conflict of Interest: There are no conflicts of interest to the authors
Source of funding: None
References
- Chaudhary M, Baisakhiya N. Clinicopathological and Radiological Study of Thyroid Swelling. Indian J Otolaryngol Head Neck Surg 2019;71(Suppl 1): 893-904. PMID: 31742091
- Khan YS, Farhana A. Histology, Thyroid Gland. StatPearls Publishing LLC. PMID: 31869123 Bookshelf ID: NBK551659
- Tamhane S, and Gharib H. Thyroid nodule update on diagnosis and management. Clin Diabetes Endocrinol 2016;2:17. PMID: 28702251
- Suresh KP, Chandrasekhar S. Sample Size estimation and Power analysis for Clinical research studies. J Hum Reprod Sci 2012;5(1):7-13. PMID: 22870008
- Riffenburgh RH. Statistics in Medicine, 2nd Edition, Academic press, 2005:85-125. ISBN: 9780080541747
- Agrawal S. Diagnostic accuracy and role of fine needle aspiration cytology in management of thyroid nodules. Journal of Surgical Oncology 1995;58(3):168–172. PMID: 7898112
- Bakhos R, Selvaggi SM, Dejong S, Gordon DL, Pitale SU, Herrmann M, et al. Fine-needle aspiration of the thyroid: rate and causes of cytohistopathologic discordance. Diagnostic Cytopathology 2000;23(4):233–237. PMID: 11002362
- Morgan JL, Serpell JW, Cheng MSP. Fine-needle aspiration cytology of thyroid nodules: how useful is it?. ANZ J Surg juill 2003;73(7):480–483. PMID: 12864820
- Gupta M, Gupta S, and Gupta VB. Correlation of Fine Needle Aspiration Cytology with Histopathology in the Diagnosis of Solitary Thyroid Nodule. Journal of Thyroid Research Volume 2010; Article ID: 379051
- Tabaqchali MA, Hanson JM, Johnsont SJ, Wadehrat V, Lennard TW, Proud G. Thyroid aspiration cytology in Newcastle: a six year cytology/histology correlation study. Ann R Coll Surg Engl 2000;82(3):149-155. PMID: 10858674
- Rout K, Ray CS, Behera SK, Biswal R. A Comparative Study of FNAC and Histopathology of Thyroid Swellings. Indian J Otolaryngol Head Neck Surg 2011;63(4):370–372. PMID: 23024944
- Yoo C, Choi HJ, Im S, Jung JH, Min K, Kang SK, et al. Fine needle aspiration cytology of thyroid follicular neoplasm, cytohistologic correlation and accuracy. Korean J Pathol 2013;47(1):61-66. PMID: 23483732
- Rao K, and Goyal VP. Comparative study of FNAV and excisional biopsy in thyroid swelling. Indian J Otolaryngol Head Neck Surg 2010;62(4):415-416. PMID: 22319704
- Bagga PK, Mahajan NC. Fine needle aspiration cytology of thyroid swellings: how useful and accurate is it? Indian J Cancer 2010;47(4):437-442. PMID: 21131759
- Grant WK. Fine needle aspiration biopsy of thyroid, neck mass & lymph node mass, primary case. J Laryngol Otol 1986;3:544–564.
- Cesur M, Corapcioglu D, Bulut S, Gursoy A, Yilmaz AE, Erdogan N, et al. Comparison of palpation-guided fine-needle aspiration biopsy to ultrasound-guided fine-needle aspiration biopsy in the evaluation of thyroid nodules. Thyroid 2006;16(6):555–561. PMID: 16839257
- Ylagan LR, Farkas T, Dehner LP. Fine Needle Aspiration of the Thyroid: A cytologic correlation and study of Discrepant cases. Thyroid 2004;14(1):35-41. PMID: 15009912
- Handa U, Garg S, Mohan H, Nagarkar N. Role of fine needle aspiration cytology in diagnosis and management of thyroid lesions: A study on 434 patients. Journal of Cytology 2008;25(1):13-17. DOI: https://doi.org/10.4103/0970-9371.40652
![]() This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑Non-Commercial‑ShareAlike 4.0 International License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑Non-Commercial‑ShareAlike 4.0 International License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.