Assess the effectiveness of structured of teaching programme on knowledge and practice regarding self-care management among chronic renal failure patients undergoing Hemodialysis at Kuppam
Year: 2025; Volume: 5; Issue: 2; Page No: 9 – 14
Article Type: Original Article
Authors: Daniel Arun Kumar1*![]() , Abhirami M2, Sumitha Devi3, Sreedevi TK4
, Abhirami M2, Sumitha Devi3, Sreedevi TK4![]() , Pavithra MN5, Melvin David6, Anagha Salikumar7, Anet Anna Benny8, Animol Paulose9, Anmaria Eldhose10, Annu Joseph11
, Pavithra MN5, Melvin David6, Anagha Salikumar7, Anet Anna Benny8, Animol Paulose9, Anmaria Eldhose10, Annu Joseph11
![]() https://doi.org/10.55349/ijmsnr.202552914
https://doi.org/10.55349/ijmsnr.202552914
Affiliations:
1Professor, Department of Medical Surgical Nursing, PES College of Nursing, Andhra Pradesh
2Professor, 3Professor, Department of Medical-Surgical Nursing, PES College of Nursing, Andhra Pradesh
4Associate Professor, Department of Mental Health Nursing, PES College of Nursing, Andhra Pradesh
5Associate Professor, Department of Obstretics & Gynaecology Nursing, PES College of Nursing, Andhra Pradesh
6Assistant Professor, Department of Community Health Nursing, PES College of Nursing, Andhra Pradesh
7, 8, 9, 10, 11 4th Year B.Sc. Nursing Students, PES College of Nursing, Andhra Pradesh
| How to cite this article: Daniel AKK, Abhirami M, Devi S, Sreedevi TK, Pavithra MN, David M, Thomas A, Priya AS, Benny A, James A, Saju A. Assess the effectiveness of structured teaching programme (STP) on Knowledge and Practice regarding self-care management among chronic renal failure patients undergoing Hemodialysis at Kuppam. Int J Med Sci and Nurs Res 2025;5(2):9–14. DOI: https://doi.org/10.55349/ijmsnr.202552914 |
Corresponding Author:
Prof. K. Daniel Arun Kumar,
Professor, Department of Medical Surgical Nursing,
PES College of Nursing,
Kuppam, Andra Pradesh, India.
Email ID: samuraidaniel432@gmail.com
Article Summary: Submitted: 05-April-2025 Revised: 30-April-2025 Accepted: 25-May-2025 Published: 30-June-2025
Abstract
Background: Chronic kidney disease (CKD) is a progressive condition characterized by impaired kidney function or structural damage that persists for more than three months. This study aimed to assess the effectiveness of a structured teaching programme on knowledge and practice regarding self-care management among chronic renal failure (CRF) patients undergoing hemodialysis at PES General Hospital, Kuppam. Andhra Pradesh.
Methods: A quantitative, pre-experimental one-group pre-test post-test design was used. A total of 40 CRF patients were selected using a convenience sampling technique. Data were collected through a structured questionnaire and checklist.
Results: Demographically, 57.5% of participants were aged between 46–65 years, 85% were male, and 75% lived in rural areas. In the pre-test,57.5%hadmoderateknowledge,and70%demonstrated adequate practice. Following the intervention, 90% had adequate knowledge and 97.5% had adequate practice. The mean knowledge score improved from 17.03 (SD=5.916) in the pre-test to 24.55 (SD=4.018) in the post-test. Statistical analysis showed a significant improvement in both knowledge and practice scores post-intervention.
Conclusion: The findings suggest that structured teaching programmes are effective in enhancing self-care management among CRF patients on hemodialysis.
Keywords: chronic renal failure, self-care management of CRF, Kuppam
Full Test
Introduction
Chronic kidney disease (CKD) is characterized by either kidney damage or an estimated glomerular filtration rate (eGFR) below 60 ml/min/1.73 m² that persists for three months or longer, regardless of the underlying cause. This condition involves a gradual decline in kidney function, which can eventually necessitate renal replacement therapy, such as dialysis or a kidney transplant. Kidney damage is identified through pathological abnormalities that may be indicated by imaging studies, renal biopsy, abnormal urinary sediment, or increased urinary albumin excretion rates. The 2012 KDIGO CKD classification provides detailed information about the cause of CKD and categorizes it into six stages based on glomerular filtration rate (G1 to G5, with G3 further divided into G3a and G3b). Additionally, CKD staging includes three levels of albuminuria (A1, A2, and A3), with each stage further classified according to the urinary albumin-creatinine ratio (mg/gm or mg/mmol) from an early morning “spot” urine sample. [1] In the United States, over 500,000 individuals live with end-stage renal disease (ESRD). The progression from chronic kidney disease (CKD) to this advanced stage is a major contributor to diminished quality of life and early mortality. CKD is a severe condition, and standard medical care includes rigorous monitoring for disease progression and early specialist referrals for dialysis or potential kidney transplantation. According to the Kidney Disease Improving Global Outcomes (KDIGO) foundation guidelines, CKD is defined by markers of kidney damage, particularly those indicating proteinuria and glomerular filtration rate. CKD is diagnosed when both a glomerular filtration rate (GFR) of less than 60 mL/min and gram of creatinine are present, along with structural or functional kidney abnormalities for more than three months. End-stage renal disease is characterized by a GFR of less than 15 mL/min. [2] Self‐care training programs improve quality of life of the patients and their families and increase their participation in self‐care programs. 17 These programs help patients to improve their self‐care abilities and personal commitment to their own health, leading to greater awareness and sound decisions about therapies and life changes, which can increase their emotional and physical well‐being. 18 With the advancements in technology, virtual education can now be accompanied by text, voice, pictures and films, making it more accessible to patients. Social media have proven to be useful for exchanging health materials between patients and health professionals. [3] Comorbidities like low hemoglobin levels, diabetes, hypertension, dyslipidemia, and thyroid disorders can significantly diminish patients’ quality of life. This highlights the importance of patient counseling, which helps patients understand the necessary lifestyle modifications to reduce preventable comorbidities. [4], [5] Objectives of the study to assess the pre-test and post-test level of knowledge and practice, to assess the effectiveness of STP by comparing pre-test and post-test level of knowledge and practice and to associate the pre-test level of knowledge and practice with their selected demographic variables
Materials and Methods
An Quantative pre-experimental study was conducted in December 2024 among 40 CRF patient who is undergoing hemodialysis in dialysis unit at PES Hospital were selected by using convenient sampling technique, informed consent were taken before the study, patients knowledge and practice were assessed by using structured self-administered questionnaire.
This includes demographic variables and Questionnaire on knowledge and practice regarding self-care management of chronic renal failure.
Statistical Analysis: Collected data were entered and complied using Microsoft Excel 2013 and data were analyzed using SPSS 14.0 version [SPSS, IBM USA Ltd.] Categorical data were presented as frequency and proportions. Continuous variables were presented as mean and standard deviation. Chi-Square test was used.
Results
The demographic characteristics of coronary artery disease (CAD) patients. as shown in Table-1.
| S. No | Demographic Variables | Classifications | No. of Patients | Percentage |
| 1 | Age Groups | a) 15 -25 Years | 3 | 7.5 |
| b) 26 – 35 Years | 4 | 10.0 | ||
| c) 36 – 45 Years | 10 | 25.0 | ||
| d) 46 – 65 Years | 23 | 57.5 | ||
| 2 | Gender | a) Male | 34 | 85.0 |
| b) Female | 6 | 15.0 | ||
| 3 | Educational Status | a) Illiterate | 9 | 22.5 |
| b)Primary education | 11 | 27.5 | ||
| c) Secondary Education | 12 | 30.0 | ||
| d) Higher Secondary Education | 3 | 7.5 | ||
| e)Under graduation | 3 | 7.5 | ||
| f)Post-Graduation | 2 | 5.0 | ||
| 4 | Occupation | a) Sedentary worker | 5 | 12.5 |
| b) Moderate Worker | 16 | 40.0 | ||
| c) Heavy Worker | 19 | 47.5. | ||
| 5 | Religion | a) Hindu | 33 | 82.5 |
| b) Muslim | 6 | 15.0 | ||
| c) Christian | 1 | 2.5 | ||
| 6 | Area of Residence
Dietary Pattern |
a) Rural | 30 | 75.0 |
| b) Urban | 10 | 25.0 | ||
| a) vegetarian | 2 | 5.0 | ||
| 7 | Dietary pattern
Duration of illness |
b) Non-vegetarian | 38 | 95.0 |
| a) <1 year | 14 | 35.0 | ||
| 8 | Habits | b) 1.1 to 3 years | 9 | 22 .5 |
| c) 3.1 to 5 years | 12 | 30.0 | ||
| d)>5 years | 5 | 12.5 | ||
| 9 | Type of access | a) AVF | 35 | 87.5 |
| b) AVG | 0 | 0 | ||
| c) IJC | 3 | 7.5 | ||
| d) SC | 1 | 2.5 |
| 10 | Frequency of dialysis per week | a) 1 Dialysis | 1 | 2.5 |
| b) 2 Dialysis | 15 | 37.5 | ||
| c) 3 Dialysis | 24 | 60.0 | ||
| d) >3 Dialysis | 0 | 0 | ||
| 11 | Co-morbid condition if any specify | a) Hypertension | 16 | 40.0 |
| b) No | 23 | 57.5 | ||
| c) Yes Hypertension and diabetes | 1 | 2.5 | ||
| 12 | Previous knowledge regarding self-care management of CRF | a)Yes | 2 | 5 |
| b)No | 38 | 95.0 |
Table-2 Frequency and percentage distribution of the pre-test level of knowledge among CRF patients (N=40)
| Level of Knowledge | Frequency | Percentage |
| Adequate Knowledge | 13 | 32.5 |
| Moderate Knowledge | 23 | 57.5 |
| In adequate Knowledge | 4 | 10.0 |
23 (57.5%) chronic renal failure patient were had moderate knowledge, 13 (32.05%) were had adequate Knowledge and 4 (10.0%) were had inadequate Knowledge. [Table – 2]
Table-3 Frequency and percentage distribution of the post-test level of knowledge among CRF Patients (N=40)
| Level of Knowledge | Frequency | Percentage |
| Adequate Knowledge | 36 | 90.0 |
| Moderate Knowledge | 4 | 10.0 |
| In adequate Knowledge | 0 | 0 |
Majority 36 (90.0%) chronic renal failure patient were had Adequate knowledge, 4 (10.0%) were had Moderate Knowledge. [Table – 3]
Figure–1 Comparison of frequency and percentage distribution of pre-test and post-test level of Knowledge among of the CRF patients
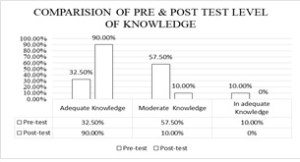
Table: 4 – Frequency and percentage distribution of the pre-test level of practice among CRF patients
| Level of Knowledge | Frequency | Percentage |
| Adequate Practice | 28 | 70.0 |
| Inadequate Practice | 12 | 30.0 |
Majority 28 (70%) chronic renal failure patient were had adequate practice, 12 (30%) were had in adequate practice.
Table: 5 – Frequency and percentage distribution of the post-test level of practice among CRF patients
| Level of Knowledge | Frequency | Percentage |
| Adequate Practice | 39 | 97.5 |
| Inadequate Practice | 1 | 2.5 |
Table – 6 Association of pre-test level of knowledge among CRF patients with their selected demographic variables
|
S. No |
Demographic Variables |
Classifications
|
Level of Knowledge | Chi-square Value |
p-Value |
||
| In adequate Knowledge | Moderate Knowledge | Adequate knowledge | |||||
| 1 | Age Groups | a) 15 -25 Years | 1 | 0 | 2 | 8.609 | 0.197
NS |
| b) 26 – 35 Years | 0 | 4 | 0 | ||||
| c) 36 – 45 Years | 1 | 7 | 2 | ||||
| d) 46 – 65 Years | 2 | 12 | 9 | ||||
| 2 | Sex | a) Male | 2 | 20 | 12 | 4.457 | 0.108
NS |
| B) Female | 2 | 3 | 1 | ||||
| 3 | Educational status | a) Illiterate | 0 | 3 | 6 | 6.582 | 0.254
NS |
| b) Primary education | 2 | 7 | 2 | ||||
| c) Secondary education | 2 | 9 | 1 | ||||
| d) Higher secondary education | 0 | 1 | 2 | ||||
| e) Under graduate | 0 | 1 | 2 | ||||
| f) Post graduate | 0 | 2 | 0 | ||||
| 4 | Occupation | a) Sedentary Worker | 0 | 3 | 2 | 0.715 | 0.949
NS |
| b) Moderate Worker | 2 | 9 | 5 | ||||
| c) Heavy Worker | 2 | 11 | 6 | ||||
| 5 | Religion | a) Hindu | 4 | 20 | 9 | 4.585 | 0.333
NS |
| b) Muslim | 0 | 2 | 4 | ||||
| c) Christian | 0 | 1 | 0 | ||||
| 6 | Area of Residence | a) Rural | 4 | 15 | 11 | 3.148 | 0.207
NS |
| b) Urban | 0 | 8 | 2 | ||||
| 7 | Dietary Pattern | a) Vegetarian | 0 | 2 | 0 | 1.556 | 0.459
NS |
| b) Non vegetarian | 4 | 21 | 13 | ||||
| 8 | Duration of illness | a) <1 year | 3 | 4 | 7 | 9.665 | 0.139
NS |
| b) 1.1 to 3 years | 1 | 7 | 1 | ||||
| c) 3.1 to 5 years | 0 | 8 | 4 | ||||
| d)>5 years | 0 | 4 | 1 | ||||
| 9 | Type of Access | a) AVF | 3 | 21 | 11 | 6.036 | 0.419
NS |
| b) AVG | 1 | 0 | 2 | ||||
| c) IJC | 0 | 1 | 0 | ||||
| d) SC | 0 | 1 | 0 | ||||
| e) FC | 0 | 0 | 0 | ||||
| 10 | Frequency of dialysis per week | a) 1 Dialysis | 0 | 0 | 1 | 2.498 | 0.645
NS |
| b) 2 Dialysis | 1 | 9 | 5 | ||||
| c) 3 Dialysis | 3 | 14 | 7 | ||||
| d) >3 Dialysis | 0 | 0 | 0 | ||||
| 11 | Co-morbid condition if any specify | a) Hypertension | 4 | 8 | 4 | 11.338 | 0.183
NS |
| b) No | 0 | 14 | 9 | ||||
| c) Yes Hypertension and diabetes | 0 | 1 | 0 | ||||
| 12 | Previous knowledge regarding self-care management of CRF | a)Yes | 0 | 1 | 1 | 0.430 | 0.807
NS |
| b)No | 4 | 22 | 12 | ||||
Table: 7 Association of pre-test level of practice among CAD patients with their selected demographic variables
|
S.No |
Demographic variables |
Classifications | Level of Practice | Chi-square Value | p-Value | |
| In adequate Practice | Adequate Practice | |||||
| 1 | Age | a) 15 -25 Years | 1 | 2 | 0.945 | 0.814
NS |
| b) 26 – 35 Years | 2 | 2 | ||||
| c) 36 – 45 Years | 3 | 7 | ||||
| d) 46 – 65 Years | 6 | 17 | ||||
| 2 | Sex | a) Male | 11 | 23 | 0.598 | 0.405
NS |
| b) Female | 1 | 5 | ||||
| 3 | Educational status | a) Illiterate | 2 | 7 | 6.582 | 0.254
NS |
| b) Primary education | 4 | 7 | ||||
| c) Secondary education | 3 | 9 | ||||
| d) Higher secondary education | 0 | 3 | ||||
| e) Under graduate | 1 | 2 | ||||
| f) Post graduate | 2 | 0 | ||||
| 4 | Occupation | a) Sedentary Worker | 3 | 2 | 7.014 | 0.030
S* |
| b) Moderate Worker | 7 | 9 | ||||
| c) Heavy Worker | 2 | 17 | ||||
| 5 | Religion | a) Hindu | 10 | 23 | 2.843 | 0.241
NS |
| b) Muslim | 1 | 5 | ||||
| c) Christian | 1 | 0 | ||||
| 6 | Area of Residence | a) Rural | 4 | 26 | 15.873 | 0.000
S* |
| b) Urban | 8 | 2 | ||||
| 7 | Dietary Pattern | a) Vegetarian | 0 | 2 | 0.902 | 0.485
NS |
| b) Non vegetarian | 12 | 26 | ||||
| 8 | Duration of illness | a) <1 year | 6 | 8 | 11.927 | 0.008
S* |
| b) 1.1 to 3 years | 0 | 9 | ||||
| c) 3.1 to 5 years | 2 | 10 | ||||
| d)>5 years | 4 | 1 | ||||
| 9 | Type of Access | a) AVF | 10 | 25 | 2.812 | 0.422
NS |
| b) AVG | 2 | 1 | ||||
| c) IJC | 0 | 1 | ||||
| d) SC | 0 | 1 | ||||
| e) FC | 0 | 0 | 3.175 | 0.204
NS |
||
| 10 | Frequency of dialysis per week | a) 1 Dialysis | 1 | 0 | ||
| b) 2 Dialysis | 3 | 12 | ||||
| c) 3 Dialysis | 8 | 16 | ||||
| d) >3 Dialysis | 0 | 0 | ||||
| 11 | Co-morbid condition if any specify | a)Hypertension | 3 | 13 | 4.810 | 0.307
NS |
| b) No | 9 | 14 | ||||
| c)Yes Hypertension and diabetes | 0 | 1 | ||||
| 12 | Previous knowledge regarding self-care management of CRF | a)Yes | 1 | 1 | 0.401 | 0.527
NS |
| b)No | 11 | 27 | ||||
The association of pre-test scores of Knowledge on Self-care management among chronic renal failure patients with their selected demographic variables such as Age, Sex, Educational Status, Occupation, Religion, Area of Residence Dietary Pattern, Duration of illness, Type of access, Frequency of dialysis per week, Comorbid condition if any specify and Previous knowledge regarding self-care management of CRF were not significant. [Table – 6]
the association of pre-test scores of Practice on self-care management among chronic renal failure patients with their selected demographic variables such as occupation, Duration of illness, was significant at the level of p<0.001 respectively Age, Sex, Educational Status, Religion, Area of residence, Dietary Pattern, Type of access, Frequency of dialysis per week, Comorbid condition if any specify and Previous knowledge regarding self-care management of CRF were not significant. [Table – 7]
Discussion
The present study was conducted to explore the knowledge and practice of self-care management among chronic renal failure (CRF) patients undergoing hemodialysis in a tertiary care hospital at Kuppam, Chittoor district, Andhra Pradesh. A descriptive and evaluative research approach was adopted. The demographic data revealed that half of patients were aged between 46–65 years, and nearly 3/4th were male. About more than 1/4th had completed secondary education, 82.5% were heavy workers, and an equal percentage followed the Hindu religion. A majority resided in rural areas, 95.0% were non-vegetarian, and 1/4th had a duration of illness less than one year. Most patients had AVF access for dialysis, and few were undergoing dialysis once daily and more than half reported no comorbid conditions. In the pre-test, more than ½th of CRF patient has demonstrated moderate knowledge, more than 1/4th had adequate knowledge, and few had inadequate knowledge. Post-test results showed significant improvement, with 90.0% of patients attaining adequate knowledge and few demonstrating moderate knowledge; none had inadequate knowledge. Regarding self-care practices, pre-test results indicated nearly 3/4th had adequate practice, which increased to 3/4th in the post-test. Only very few exhibited inadequate practice post-intervention. Statistical analysis showed no significant association between pre-test knowledge scores and demographic variables such as age, sex, education, occupation, religion, residence, diet, and duration of illness, type of access, dialysis frequency, comorbidities, or prior knowledge. However, practice scores showed a statistically significant association with occupation and duration of illness (p<0.001).
These findings are supported by a similar study conducted by Ahmed SH and Abd Elzaher OM, [6] which evaluated the effect of a structured teaching programme on knowledge and self-management behaviours among hemodialysis patients. In their study, only 17% of patients had satisfactory knowledge in the pre-test, which significantly increased to 93% in the post-test. A statistically significant improvement was noted in self-management behaviours following the implementation of the structured programme (p<0.001).
Conclusion
This study revealed that most chronic renal failure (CRF) patients undergoing hemodialysis in the tertiary care hospital had moderate knowledge and adequate practice in self-care management during the pre-test phase. The structured teaching program significantly improved their knowledge and practice, as evident from the post-test results, with 90% achieving adequate knowledge and 97.5% demonstrating adequate practice. Demographic factors showed no significant association with knowledge, while occupation and duration of illness had a significant association with practice scores. The findings underscore the effectiveness of educational interventions in enhancing self-care management among CRF patients. This highlights the need for continued education to empower patients in managing their condition effectively.
Source of funding: None
Conflict of Interest: Nothing to declared by the authors
Acknowledgement: We acknowledge all the CRF patients who actively participated in the study.
Authors’ Contributions: All authors conceived and designed the article. Wrote the full paper and checked by all the authors.
References
- Vaidya SR, Aeddula NR. Chronic Kidney Disease. 2022 Oct 24. In: Stat Pearl. Treasure Island (FL): Stat Pearls Publishing; 2024. PMID:
- Hashmi MF, Benjamin O, Lappin SL. End-Stage Renal Disease. 2023. In: Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing; 2024. PMID:
- Tashakor S, Bagherian B, Salmanpour Z, Mehdipour-Rabori R. The effect of a training program on the self-care efficacy of hemodialysis patients with mineral and bone disorders: A quasi-experimental study. Health Sci Rep 2023;6(7):e1429. DOI: https://doi.org/10.1002/hsr2.1429 PMID: 37448728; PMCID: PMC
- Linda S. Williums, Paula D. Hopper, “understanding medical surgical nursing’’ 4th edition JAYPEE Medical Publisher Pvt. Ltd. pp:859- 864.
- Javed Ansari, Davinder Kaur, “textbook of medical surgical nursing-1, Medical Publisher. pp852- 868
- Shymaa H. Ahmed 1 Omima M. Abd Elzaher 2 Hanaa Esmail Sabra structured teaching programme‘s effect on knowledge and self-management behaviors for hemodialysis patients. DOI: https://doi.org/10.21608/TSNJ.2021.198903 Vol 2 2021.
![]() This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑Non-Commercial‑ShareAlike 4.0 International License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given, and the new creations are licensed under the identical terms.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑Non-Commercial‑ShareAlike 4.0 International License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given, and the new creations are licensed under the identical terms.