![]()
Article Type: Short Communication
Multivariate Logistic Regression Models in the Progression of Vision Threatening Disease
Year: 2023; Volume: 3; Issue: 3; Page No: 16 – 19
Authors: Senthilvel Vasudevan![]()
![]() https://doi.org/10.55349/ijmsnr.2023331619
https://doi.org/10.55349/ijmsnr.2023331619
Affiliations: Assistant Professor in Statistics (Biostatistics), Department of Community Medicine, Sri Venkateshwaraa Medical College Hospital & Research Centre, Ariyur, Pondicherry – 605 102. Email ID: senthilvel99@gmail.com
| How to cite this article: Vasudevan S. Multivariate Logistic Regression Models in the Progression of Vision Threatening Disease. Int J Sci and Med Res 2023;3(3):16-19. |
Article Summary: Submitted: 10-July-2023; Revised: 12-August-2023; Accepted: 05-September-2023; Published: 30-September-2023
Abstract
Diabetic Mellitus is a disease of inadequate control of level of glucose in blood. It is also happened by disorder of carbohydrate metabolism by impaired ability to produce insulin in blood. In this article, I have to discuss about how to find risk factors and how much its influence in the progression of Diabetic Retinopathy (DR), to identify the presence of DR and its progression by formulating some mathematical equations with suitable variables and to find several stages of DR and its progression. The continuous variables were expressed as mean and standard deviation and categorial variables as frequency and proportions. In this, we have discussed about various kind of statistical prediction models.
Found the influencing factors in the progression of DR by using multiple logistic regression analysis, predicted the probability of a DM patient in the progression of DR and found the probability of DR among diabetes up to a given period of time and using by Markov Chain Analysis found the TPM and the absorbing state in a DM patient and to identify as having complete vision loss.
I have concluded that the statistical models were explained and found the influenced factors and risk ratio to develop DR among DM patients has been computed, and transition of DR which predict the chance to develop DR in a DM patient and found the probability to develop DR over a period of time has also explained via procedure.
Keywords: diabetic mellitus, diabetic retinopathy, statistical models, risk ratio
Corresponding Author:
Dr. Senthilvel Vasudevan, Ph.D.,
Assistant Professor in Statistics (Biostatistics),
Department of Community Medicine,
Sri Venkateshwaraa Medical College Hospital & Research Centre,
Ariyur, Pondicherry – 605 102. India.
Email ID: senthilvel99@gmail.com
Main Text
Introduction
Diabetic Mellitus is a disease of inadequate control of level of glucose in blood. It is also happened by disorder of carbohydrate metabolism by impaired ability to produce insulin in blood. DM affects about 180 million people in the presently and it is a public health problem in worldwide. DM causes majorly blindness, kidney failure, heart attacks, stroke, and lower limb amputation. Increase of 3% DM mortality by age in between 2000 and 2019 years. Moreover, there was an estimated 2 million deaths due DM and kidney disease. [1] Diabetes symptoms may occur suddenly or if it is mild then it may notice after some years. DM symptoms are feeling very thirsty, needing to urinate more often than usual, blurred vision, feeling tired and losing weight unintentionally. After a long period time, DM can damage blood vessels in heart, eyes, kidney and nerves. There are three types of DM are, Type-1 DM, Type-2 DM and Gestational DM. [2] Type-I DM is caused an autoimmune reaction. This is stopping the insulin making in a person. 5 – 10% of people have affected by diabetes with type-I; In Type-1 DM, a person body doesn’t use insulin well and can’t keep blood sugar level at normal. This type of DM is in 90 – 95% of people in world level; and Gestational DM develops in pregnant women who have never had diabetes. Usually, GDM has gone away after the baby born. Diabetes causes Diabetic Nephropathy in diabetes patients. [3]
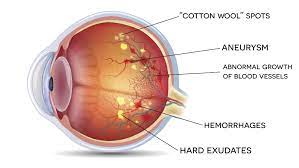
Diabetic Retinopathy (DR) is a major complication of DM. It is a microvascular complication of DM. DR is also called “Vision Threatening Disease (VTD)”. [4] In year 1990, as per WHO report revealed that 4.58% global total population has change in prevalence of visual impairment; in that 55% of visually impaired people are women; 89% of visually impaired people those who are live in low- and middle-income countries. Globally, 1.1 billion people with near-vision impairment. As per WHO, in the year 2019 global target to reduce the prevalence of avoidable visual impairment by 25%. Globally, nearly 2.2 billion people have a vision impairment. [5] One third of times more chance of getting blindness in diabetics than non-diabetics. DR is causing vision loss in worldwide and nearly three fourth of population were affected those who were living in under developing income countries. DR is a very worst difficulty and all parts of diabetic eye will be affected as shown in [Figure-1].
Figure – 1 View of eye affected by diabetic retinopathy
Main factors for development of DR are duration of DM, glycemic control, age, sex, high blood pressure, kidney diseases, heredity, lipids profiles, malnutrition, puberty, poverty, pregnancy. Duration of DM and glycemic control had direct and indirect correlation with DR. Hypertension is also an increasing risk of DR in T2DM patients. In this article, I have discussed how to find out the risk factors and how much its influence in the development of DR, to identify the risk factors that influencing in the progression of DR, to identify the presence of DR and its progression by forming mathematical equations using which was found possible development of DR with some variables and to find the several stages of DR and its progression over a period of time (in years).
Various Types of Statistical Models used in the progression of DR:
Multivariable Logistic Regression [6, 7] Y = OCT value (in µm) is to be taken as dependent variable. The independent variables are to be collected as per the availability of data. In this model, Age taken as X1 (in years), Gender(X2): Male = 1, Female = 0, HbA1C as X3 (%), Duration of DM as X4 (in years), Triglyceride as X5 (mg/dl), HDL as X6 (mg/dl), Family History (X7) retinopathy in their family = 1, otherwise = 0, Hypertension as X8, if patient had high blood pressure = 1, otherwise 0, LDL as X9 (in mg/dl). OCT is an imaging technology which can uses low coherence light to cover micrometer resolution and imaging in biologic tissues. [8, 9] By this model, significant variables, ANOVA test for goodness of fit and R-Square value were found. F-value not significant, then the model was good fit for prediction in the development of DR. It measures macular edema thickness (MET). We could write multiple variable equation as, Y = β0 + β1 X1 + β2 X2 + … … … + β11 X11 ………… (1). Fix all values of β multiplier and to find out macular edema thickness.
Binary Logistic Regression [10 – 15] samples were collected consecutively by using simple random sampling method from the patients’ data base. In this approach Y as dependent variable. If an individual having DR then, Y = 1, otherwise = 0 (without DR). Independent variables were, Age (X1) taken as in years; Sex (X2) = 1 (male), Female = 0; HbA1C (X3); Pre-Prandial sugar level (X4); Post-Prandial sugar level (X5); Systolic Blood pressure, (X6); Diastolic Blood pressure (X7); Duration of diabetes (X8); Serum triglycerides (X9); Serum HDL-cholesterol (X10); Family History of DR (x11) = 1, otherwise = 0. Significant variables were found by bivariate Chi-Square test and the other variables with p<0.20 were included in the final BLR analysis with step-wise elimination method. By Binary Logistic Regression model, we have identified the influencing factors of DR. For goodness of fit, Hosmer-Lemeshow test was used. In H-L test, Χ2-test wasn’t significant meant the selected variables were good fitted to BLR equation.
Y = β0 + β1 X1 + β2 X2 + … … … + β11 X11 [14] ————– (1)
Substitute, x1, x2, … … …, x11 in the equation and to find ‘Y’ value and eY. Then, the odds ratio by using,
P
——– = eY ———————————— (2)
1 – P
and p–value is to be found. Hence, one could get the chance for development of DR in a DM patient.
Cox Regression Analysis, [16] recorded the patients’ difficulties like high blood pressure (X1), family history of DR (X2) and neurological disorder (X3) were taken as binary values as X1, X2 and X3. Sample were collected by simple random sampling with inclusion criteria those who were had the above mentioned 3 problems with certain aged (in years) and those who were living one year and above in a particular area/region. Exclusion criteria of those weren’t have the above-mentioned problems and any other heart problems/complications. If a patient had no problem, then covariate taken (0, 0, 0) and hand all (1, 1, 1). Totally there were eight covariate combinations (1,1,1), (1,0,1), (0,1,0), (0,0,1), (0,1,1), (1,0,0), (1,1,0), and (0,0,0). To find β1, β2, and β3 by solving Cox’s partial likelihood. [17]
From the above likelihood function, equations (1), (2), and (3) has been formulated and simplify, then would get the values of
^ ^ ^
β1, β2, β3 other possible covariate combinations have formed. We have to form over all probability to develop DR as:
h(t) = h0 (t) ex1β1+x2β2+x3β3+……. + xkβk
In this, h(t) denotes the overall probability of developing DR; h0(t) denotes the hazard rate due to past duration of diabetes and ex1β1+x2β2+x3β3+… …+xkβk is the overall hazard rate based on respective DR patient’s Covariate combinations. By solving the above equation, then we would get the probability of developing DR up to over a period of time of a T2DM patient.
Markov Chain Analysis [18] conducted a DR patients were collected from hospital for two consecutive years patient’s records by simple random sampling method with an inclusion criteria in age and some other, an exclusion of those who were had other severe diseases and not willing to participate in our study. At every visit, a retinal specialist graded retinal findings using a modification of the Airlie House Classification of Diabetic Retinopathy (AHCDR). [19] AHCDR is the gold standard method on grading of stereo photographs of 7 fields and classifies DR into 13 complex levels ranging from level 10 (no DR) to 85 (severe vitreous hemorrhage). Patients were screened first time in first year, and the second screen was done after one year in next consecutive year to the same patients and found their DR stages. The four-stages of Markov Chain model for the natural course of DR. [20] Markov model is a time-homogeneous distribution by using this estimating transition probabilities, and the mathematical symbols for transition probabilities was generated. I have classified NPDR into further classifications and formed six-stages of MC model for the natural progress of DR. I have taken, stage-1 indicates no retinopathy; stage-2 as micro aneurysms, stage-3 and 4 indicate intermediate stages of background DR, stage-5 as pre-proliferative and stage-6 proliferative retinopathy. Like this, we could formulate the transition rate matrix and its probability matrix for six-stages of DR. From this, we have got the probability of developing DR in a person for 1 and 5 years by forming both transition matrix and TPM.
Conclusion
From this statistical models’ studies, the influencing factors for the development of DR from this one individual can identified their risk factors. The risk ratio has been computed which predict the chance of the development of DR of a T2DM patient. The number of years of DM is a prominent risk factor of the development of DR in a T2DM patient. The progression and transition of DR were increased by increasing by the duration of DM. A known diabetes patient can understand about the significant risk factors, how to reduce their severity of stages of DR or to retain/protect in their same stage. So, undergo regular checkups every six for their affected eye with a trained ophthalmologist in a well-equipped eye hospital. Further studies have to be conducted related to these models with suitable sampling method and adequate samples in future.
Source of funding: None
Conflict of Interest: None
Authors’ Contributions: SV – Authors contributed to the conceptualization, writing of the article and in preparation and checking of the article.
Here, SV – Senthilvel Vasudevan
References
- World Health Organization: Diabetes. Available from: https://www.who.int/news-room/fact-sheets/detail/diabetes#:~:text=Diabetes%20is%20a%20major%20cause,an%20estimated%202%20million%20deaths
- Centers for Disease Control and Prevention: Diabetes Basics. Available from: https://www.cdc.gov/diabetes/basics/index.html#:~:text=Diabetes%20is%20a%20chronic%20(long,diabetes%20(diabetes%20while%20pregnant) [Last Accessed on 10th June 2023]
- Sahu S, Taywade M, Devi S, Nayak S, Dipti SM. A study of modifiable and non-modifiable risk factors associated with diabetic nephropathy – A preliminary observational study in Eastern Odisha, India. Int J Med Sci and Nurs Res 2021;1(1):17-21. DOI: https://doi.org/10.55349/ijmsnr.2021111721
- Alsolaimi YA, Almudaymigh MS,
Al Essa M, Gramish J, Bustami R, Al Yami M, Vasudevan S. Influencing factors on vision-threatening disease among patients with diabetes in the central region of Saudi Arabia: A Case-Contral Study. Journal of Fam Med and Prim Care 2022;11(6):2399-2404. DOI: https://doi.org/10.4103/jfmpc.jfmpc_601_21 - World Health Organization: World report on vision – Report 2019. Available from: https://www.who.int/docs/default-source/documents/publications/world-vision-report-accessible.pdf [Last Accessed on 15th June 2023]
- Bora A, Balasubramanian S, Babenko B, Virmani S, Venugopalan S, Mitani A. Predicting Risk of Developing Diabetic Retinopathy using Deep Learning. 2008;1–40. Available from: https://arxiv.org/ftp/arxiv/papers/2008/2008.04370.pdf
- Arcadu F, Benmansour F, Maunz A, Willis J, Haskova Z, Prunotto M, et al. Deep learning algorithm predicts diabetic retinopathy progression in individual patients. NPJ Digit Med. 2019;2:92.
- Chan A, Duker JS, Ko TH, Fujimoto JG, and Schuman JS. Normal Macular Thickness Measurements in Healthy Eyes Using Stratus Optical Coherence Tomography. Arch Ophthalmol 2006;124(2):193-198. PMID: 16476888
- Sanchez-Tocino H, Alvarez-Vidal A, Maldolnado MJ, et al. Retinal thickness study with optical coherence tomography in patients with diabetes. Invest Ophthalmol Vis Sci. 2002;43:1588–1594.
- Bender R, Grouven U. Using binary logistic regression models for ordinal data with non-proportional odds. J Clin Epidemiol 1998;51(10):809-816. PMID: 9762873
- Hussain S, Qamar MR, Iqbal MA, Ahmad A, and Ullah E. Risk factors of retinopathy in type 2 diabetes mellitus at a tertiary care hospital, Bahawalpur Pakistan. Pak J Med Sci 2013;29(2):536-539. PMID: 24353572
- Ahmed RA, Khalil SN, and Al-Qahtani MAA. Diabetic retinopathy and the associated risk factors in diabetes type 2 patients in Abha, Saudi Arabia. J Family Community Med 2016;23(1):18-24. PMID: 26929725
- Gong Di, Fang L, Cai Y, Chong I, Guo J, Yan Z, et al. Development and evaluation of a risk prediction model for diabetes mellitus type 2 patients with vision-threatening diabetic retinopathy. Front Endocrinol 2023;14. Available from: https://www.frontiersin.org/articles/10.3389/fendo.2023.1244601/full
- Vasudevan S, Senthilvel S, Sureshbabu J. Study on risk factors associated with diabetic retinopathy among the patients with type 2 diabetes mellitus in South India. International Eye Science 2017;17(9):1615-1619.
- Vasudevan S, Prasad A. A hospital based cross sectional study on determining of prevalence and risk factors of eye disease among diabetics in a teaching tertiary care hospital in India. International Journal of Medical Sciences and Nursing Research 2022;2(1):10-16. DOI: https://doi.org/10.55349/ijmsnr.2022211016
- Chen X, Xie Q, Zhang X, Lv Qi, Liu X, and Rao Huiying. Nomogram Prediction Model ofr Diabetic Retinopathy Development in Type 2 Diabetes Mellitus Patients: A Retrospective Cohort Study. J Diabetes Res 2021;2021:3825155. PMID: 34595241
- Ko J. Solving the Cox proportional Hazards Model and Its Applications. 2017 Technical Report No: UCB/EECS-2017-110. Available from: https://www2.eecs.berkeley.edu/Pubs/TechRpts/2017/EECS-2017-110.pdf [Last Accessed on: 2nd July 2023]
- Srikanth P. Using Markov Chains to predict the natural progression of diabetic retinopathy. Int J Ophthalmol 2015;8(1):132-137. PMID: 25709923
- Grading diabetic retinopathy from stereoscopic color fundus photographs–an extension of the modified Airlie House classification. ETDRS report number 10. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1991;98(5 Suppl):786-806. PMID: 2062513.
- Senthilvel V, Radhakrishnan R, Sathiyamoorthi R, Sumathi S, Jayanthi V. A Study on Multi Stages of Diabetic Retinopathy among Diabetic Patients in Puducherry – Using Markov Chain Model Approach. Advances in Applied Mathematical Biosciences 2012;3(1):49-55.
![]() This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑Non-Commercial‑ShareAlike 4.0 International License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑Non-Commercial‑ShareAlike 4.0 International License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Abstract Full-Text PDF